
Harry Partch – The Outsider Who Refused To Come In
“This is my trinity: sound-magic, visual beauty, experience-ritual.”
One of the great American myths is the cult of individualism. Individualism is sometimes twinned with the alleged American love of iconoclasts.
Those myths last until a real American iconoclastic individual comes along and starts making some noise. Actual American iconoclastic individuals are usually shunned, ignored, criticized, ridiculed and forced to the margins of society.
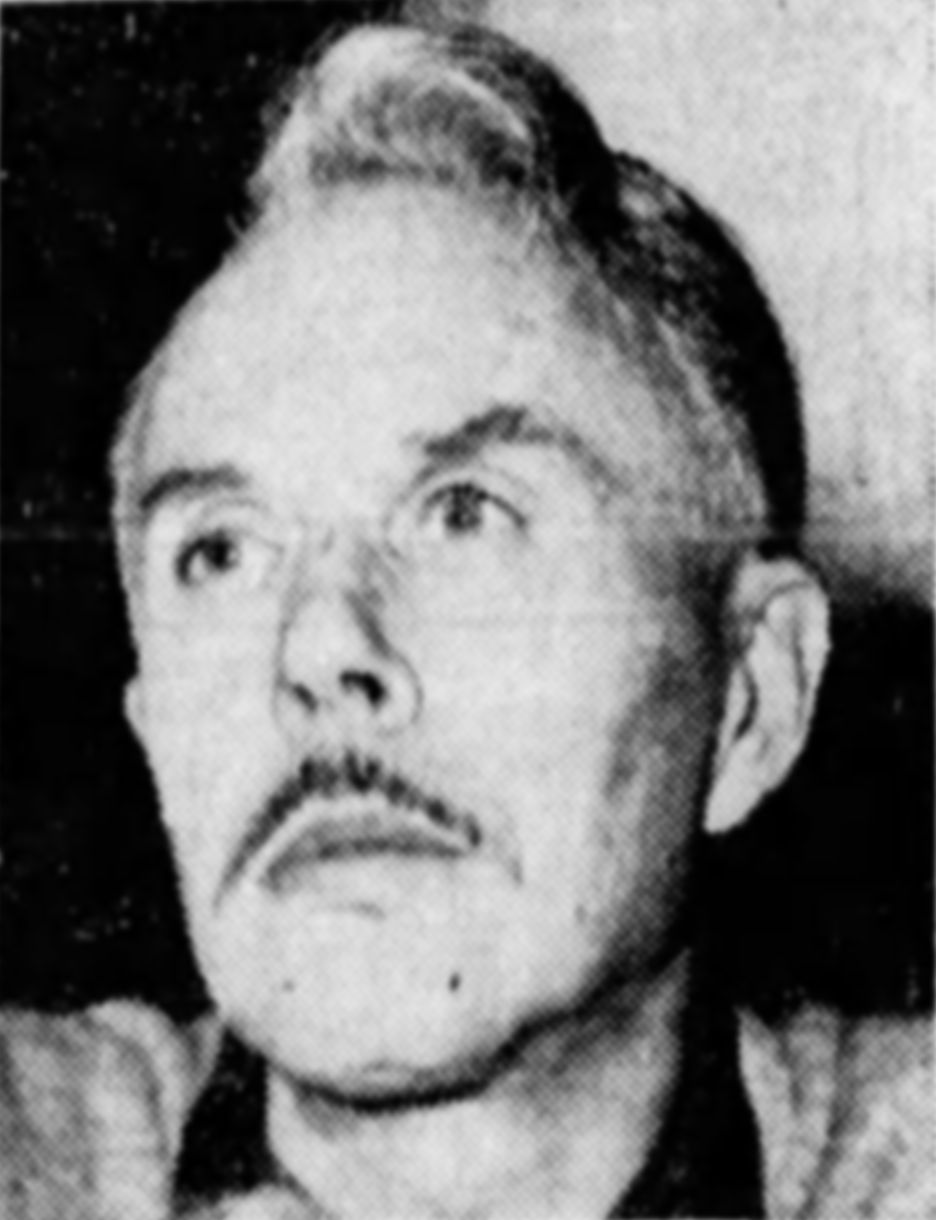
Harry Partch, The San Francisco Examiner, Sunday, March 9, 1952. Public Domain
Harry Partch, American composer, music theorist, and creator of unique musical instruments, was one of these iconoclastic individuals.
Today, 24 June 2026, would have been his 125th birthday.
You probably have never heard of Harry Parch unless you are a fan or student of obscure 20th century avant-garde music or a former listener of the now defunct radio program The Dr. Demento Show, which specialized in novelty songs, comedy, and unusual recordings and aired on radio and online from 1971 to 2025.
Parch genuinely lived life and made music on his own terms. He was a true outsider who refused to come in.
Despite the fact was always an outsider, Partch attracted the attention and respect of many musicians as well as dancers and choreographers, because his music was often paired with physical movement. His work maintains a cult following to this day, partly fueled by the fact the Dr. Demento radio show regularly played on his songs, Barstow and I Am a Peach Tree. https://www.prostudiomasters.com/album/page/99475
Partch was seemingly born to be musician and an outsider.
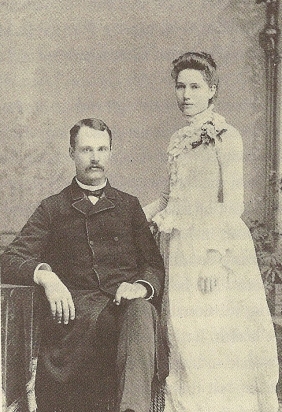
Partch’s parents, Virgil and Jennie at their wedding (1888)
Harry Partch was born 24 June 1901 in Oakland, California, son of Virgil Franklin and Jennie (née Childers) Partch, a pair of Presbyterian missionaries who proselytized in China from 1888 to 1893, and again from 1895 to 1900, until they fled the Boxer Rebellion.
Soon after Harry’s birth, his family decamped to Benson, Arizona, after his mother contracted tuberculosis mother’s health. A town of about 1,000 in Cochise County, Benson was founded as a Southern Pacific Railroad rail junction for shipping ore and supplies between mines near Tombstone, Fairbank, Contention City and Bisbee.
Arizona was still the wild west when the Partch family arrived in Benson. Arizona gained statehood in February 1912, the 48th state, and last of the contiguous states admitted to the Union.
The youngest of three siblings, Parch showed musical talent early in his life. He learned to play the mandolin, violin, piano, reed organ, and cornet. His mother taught him to read music. His older brother Paul played mandolin. His and older sister Irene played violin and cello.
Partch heard the music of the indigenous Yaqui people. His mother would sing to him in Mandarin Chinese. He heard and sang songs in Spanish.
When his family moved to Albuquerque, New Mexico, in 1913, he studied the piano seriously, and while in high school he worked playing keyboards for silent films. He was composing for the piano at 15 and he developed an early interest in writing music for dramas.
In the posthumously published “Bitter Music: Collected Journals, Essays, Introductions, and Librettos.” Partch mentions the lost composition Death and the Desert 1916 as an early musical drama work.

1919 graduation photo of American composer Harry Partch
The year 1919 brought big changes for Partch. He graduated from high school, his father died and his family moved to Los Angeles. His mother was killed, crushed to death while changing trolleys, in 1920
Partch enrolled to study piano at the University of Southern California in 1920. Dissatisfied, he left USC after the summer of 1922. He moved to San Francisco and working as a proofreader, piano teacher, and violist while continuing to compose and studing music.
In 1923, Partch discovered Hermann von Helmholtz’s Sensations of Tone, which led him to just intonation, the tuning of a musical interval without beats resulting in an acoustically pure sound.
https://en.wikipedia.org/wiki/Hermann_von_Helmholtz
https://en.wikipedia.org/wiki/Sensations_of_Tone
This would lead Partch on to blow up the 12 tone confines of western music, develop his own musical theory, building specialized instruments to play the resulting compositions.
BURNING THE WESTERN MUSICAL TRADITION
By 1925, Partch was developing paper coverings for violin and viola with fingerings in just intonation, writing a string quartet using such tunings.
He begins to write down this theories. In May 1928, he has a first draft for a book, then called Exposition of Monophony. He survived by teaching piano, proofreading, and even working as a sailor.
By 1930 he’s in New Orleans. He breaks with the European musical tradition, burning all his scores.

Partch playing the Adapted Viola, 1933. Public Domain
He has a violin maker build a viola with the fingerboard of a cello dubbed the Adapted Viola. He uses his Adapted Viola to write music using a scale with twenty-nine tones to the octave.
In 1932 Partch goes on the road, performing in San Francisco and Los Angeles with sopranos he had recruited. He beings to attract patrons. A performance at Henry Cowell’s New Music Society of California gets good reviews.
Sponsors pay for Partch to go to New York in 1933 for a series of solo performances. He’s a hit. Composers Roy Harris, Charles Seeger, Henry Cowell, Howard Hanson, Otto Luening, Walter Piston, and Aaron Copland signal their support.
Partch applies for Guggenheim grants in 1933 and 1934 but is not accepted.
The Carnegie Corporation of New York gives him a $1500 grant (about $37,000 today) to do research in England. He gives readings at the British Museum and travels Europe. In Dublin he meets poet W. B. Yeats. Partch proposes setting Yeast’s translation of Sophocles’ King Oedipus to his music. He even studies the spoken inflection in Yeats’s recitation of the text, a harbinger of his future techniques of linking the speaking voice to music.
He builds the Chromatic Organ, a keyboard instrument, using a forty-three tones to the octave scale.
He meets musicologist Kathleen Schlesinger, who recreated an ancient Greek kithara harp from images on a vase at the British Museum. He sketches the instrument in her home, discussing ancient Greek music theory with her. This is a meeting that would inspire the later building of Partch’s own kitharas and pursuit of Greek inspires musical forms.
You would be forgiven if you might think Partch sounded as if his oddball outsider music was making him a living from patrons and grants and famous in certain circles.
Returning to America 1935 at the height of the Great Depression, Partch literally took a different road.
PERSONAL LIFE
Partch’s personal life and personal philosophy were every bit as adventurous and unconventional as his music.
His family and his environment shaped his musical outlook. His sexuality helped shape him as an outsider.
Parch realized he was gay as young person. He lived about as openly as a gay man could in the early 20th century.
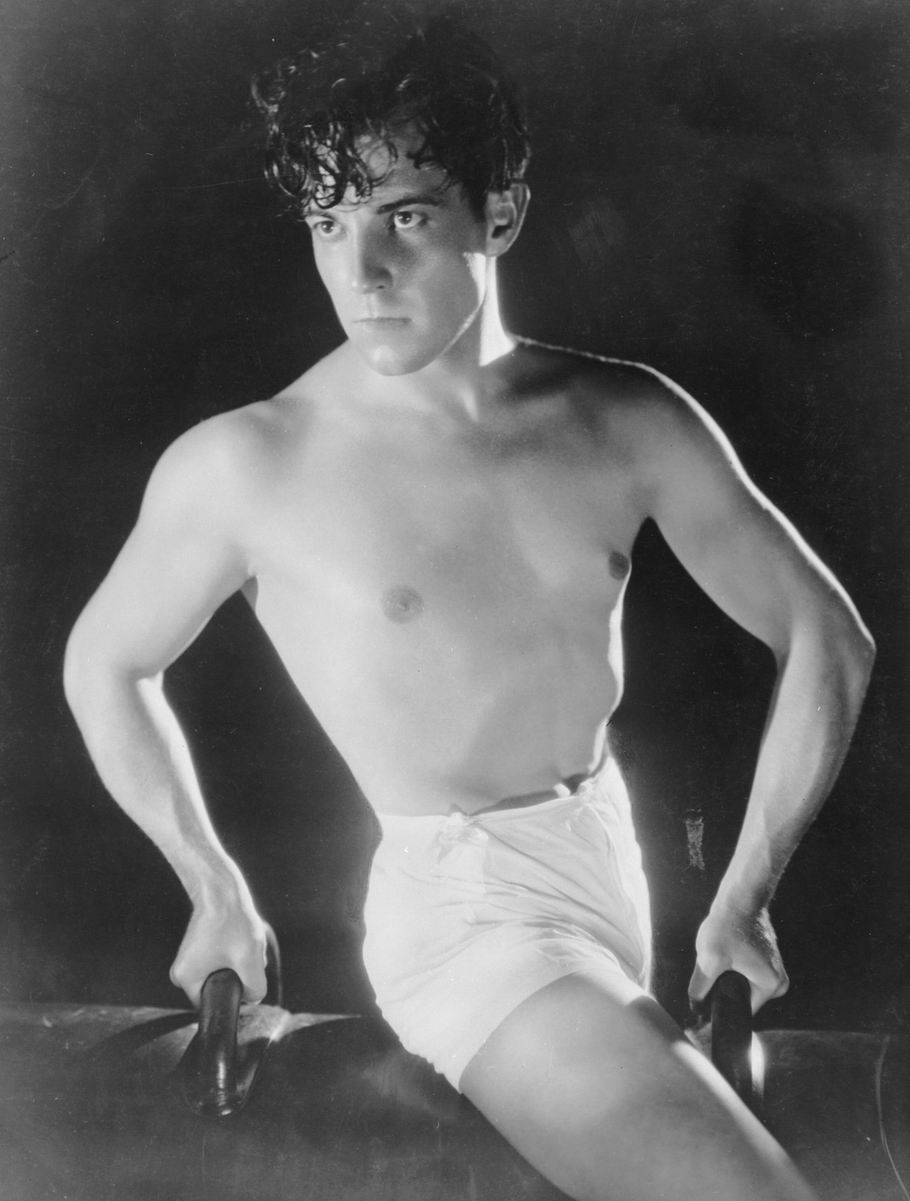
Ramón Novarro, c. 1925. Public Domain
While working as an usher for the Los Angeles Philharmonic, Partch had a romantic relationship with the actor Ramon Navarro, aka Ramón Samaniego. Navarro ended the relationship when his acting career took off after his starring role in Scaramouche (1923) brought him his first major success. Navarro would go on to become Hollywood’s leading Latin actor after Rudolph Valentino died in 1926.
https://en.wikipedia.org/wiki/Ramon_Novarro
Partch’s sexuality, however, is probably the least interesting thing about him.
He was also life-long a heavy drinker. In the 1960s he chose the location of a studio in then seedy Venice Beach in Los Angeles because of its proximity to a liquor store.
“A defiant, hard-drinking maverick who detested the musical mainstream — even the avant-garde musical mainstream (he despised John Cage) — Partch was a cantankerous man who blew up many personal and professional relationships that could have done him much good,” Tim Page, professor emeritus of musicology at the Thornton School of Music, University of Southern California, wrote in a October 2025 piece on the LA Phil website.
https://www.laphil.com/about/watch-and-listen/a-meditation-on-harry-partch-hitchhiking-and-hoboism
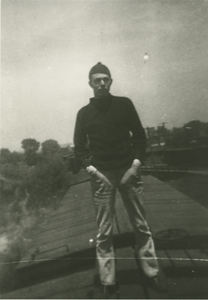
Harry Partch Standing on a Train Car ca. 1930sMusic and Performing Arts, University of Illinois at Urbana Champaign
During the height of the Great Depression, Partch mostly drops out of the music world and society in general and became what was then politely call a hobo. He spend the better part of a decade penniless, riding freight trains and hitchhiking from one end of the United States to the other and back again.
Partch led a transient life for about nine years. During his time on the road he reportedly drank heavily, “found companionship,” and contracted syphilis.
He wasn’t completely disconnected during this time because managed to compose music, build instruments, and develop his book and theories, and even make his first recordings.
Sometimes he worked or received grants from organizations such as the Federal Writers’ Project. During eight months of his life on the road, he kept a journal published posthumously as “Bitter Music.”
He built his first kithara Big Sur, California, in 1938 after taking woodworking courses. His kithara was about twice the size of Schlesinger’s kithara in England. In 1942 in Chicago, his builds a 43-tone reed organ, the Chromelodeon.
UNIVERSITY YEARS, DANCES AND FILMS
Partch pulls off the road in March 1943 when he receives a Guggenheim grant to construct instruments and write his seven-part Monophonic Cycle. On 22 April, 1944, the first performance of his Americana series takes place at Carnegie Chamber Music Hall sponsored by the League of Composers.

Harry Partch’s New Kithara I, a string instrument playing in just intonation. Photographed at the Harry Partch Institute at Montclair State University. Creative CommonsComposers.
Emerging from his hobo years, Partch set about using his Depression era experiences as creative fodder. Utilizing Guggenheim and university grants, from 1944 until 1947 Partch began a productive period at the University of Wisconsin.
He lectured, trained an ensemble, staged performances, released his first recordings, while at the University of Wisconsin. Perhaps most significantly, he finishes his book began in 1928 as “Exposition of Monophony,” and now titled “Genesis of a Music.” Completed in 1947, “Genesis of a Music” is published in 1949 by the University of Wisconsin Press.
Despite his creative time at the University of Wisconsin, Partch left the university and, maybe, it left him. He didn’t find a permanent position at the university or a place for his growing inventory of self-made instruments.
Copenhagen-born pianist and composer Gunnar Johansen, who taught at the University of Wisconsin–Madison, allowed Partch In 1949, to convert a smithy on his ranch in Blue Mounds, Wisconsin, into a studio. Partch worked in Blue Mounds, about 25 miles west of Madison, from 1949 to 1950 with financial support from the Guggenheim Foundation. There he made several recordings. most notably his Eleven Intrusions, assisted for six months by composer Ben Johnston.
Partch moved to Oakland, California, in early 1951, for health reasons.
While in Oakland, another project from his time in Europe came to fruition.

Partch (center) directing four college students in rehearsal. The San Francisco Examiner, Sunday, March 9, 1952. Public Domain
Working with designer Arch Lauterer., Partch staggered a production of Yeats’s translation of Sophocles’s play King Oedipus at Mills College in Oakland. Performances of King Oedipus took place in March 1951, receiving numerous reviews. Yeats’s estate refused to grant permission to use Yeats’s translation, nixing a planned recording.
In an abandoned shipyard in Sausalito, California, Partch opened a studio, named Gate 5, in early 1953. At Gate 5 he composed, built instruments and staged performances and established an independent record label.
The Harry Partch Trust Fund was created by friends and supporters to sell subscriptions to raise money for recording. Sold by mail order on the Gate 5 Records label, money raised from the recordings became Partch’s main source of income.
Partch’s Plectra and Percussion Dances, Ring Around the Moon (1949–1950), Castor and Pollux, and Even Wild Horses, were broadcast on Berkeley’s KPFA radio station in November 1953.
When he completed The Bewitched: A Ballet Satire, in January 1955, Partch tried to find a way to stage the work. This led to another major turning point in Partch’s life and career.
Composer Ben Johnston, who worked with Partch in Wisconsin, advocated for Partch to receive a visiting artist position at the University of Illinois in 1956.
With the help Johnston and the Fromm Foundation, The Bewitched was performed at the University of Illinois, in March 1957, and later at Washington University in St. Louis. However, Partch didn’t like choreographer Alwin Nikolais’s interpretation.
Partch provided the music for Chicago based avant-garde filmmaker Madeline Tourtelot’s film Windsong in 1957, the first of six film collaborations.
HARRY PARTCH – MadelineTourtelot/Windsong (Movie)
A 1958 Film by MadelineTourtelot , from the eastern shores of Lake Michigan.
https://youtu.be/WWjpanCFPAQ?si=SHXUheBWjeZkDaHN
HARRY PARTCH – U.S. Highball (Full Movie)
Trans-Continental Hobo account of riding the rails during the Depression. Film by Madeline Tourtelot 1958.
https://youtu.be/Xy9AtlLrYaI?si=2QsVdKD26tgVB339
Between 1959 to 1962, Partch received further appointments from the University of Illinois. He staged productions of his works Revelation in the Courthouse Park (1961) and Water! Water! (1962), both of which were based on Greek mythology.
Ben Johnston introduced Partch to Danlee Mitchell, a percussionist and University of Illinois student, later became Partch’s principal percussionist, assistant, amanuensis, Mitchell eventually became Partch’s heir and the executor of Partch’s estate.
Mitchell would later relocate to San Diego, where he would become a professor of music at San Diego State University. Partch spent the last years of his life in the San Diego County communities of Del Mar and Encinitas, while working closely with Mitchell.
After Partch’s death, Mitchell oversaw productions and maintained an ensemble that toured and performed concerts of Partch’s work.
Mitchell died 31 July 2024 in Lakeside, California of liver cancer. He was 87.
Partch had support from Mitchell and several departments and organizations at the University of Illinois. But the U of I music department hated him.
In 1962, Partch decided to leave Illinois and return to California.
DREAMING IN SOUTHERN CALIFORNIA
Late 1962, Partch set up a studio in a former chicken hatchery in Petaluma, California, Sonoma County, California, north of San Francisco. He composed two works, And on the Seventh Day and Petals Fell in Petaluma in Petaluma.
Partch departed Petaluma in summer 1964, moving to Del Mar in San Diego County for an anticipated artist in residency at the University of California at San Diego that would not actually happen for another two years.
Betty Freeman met Partch in Pasadena in 1964. Freeman was an arts patron who assisted composers Lou Harrison, John Cage, La Monte Young, Christopher Rouse, Philip Glass, Steve Reich, John Adams, Anders Hillborg, Pierre Boulez, Harrison Birtwistle, Virgil Thomson, Helmut Lachenmann, and Kaija Saariaho.
But Freeman took a special interest in Harry Partch, saying he changed her life.
Aside from Mitchell, Freeman became Partch’s most important friend, patron, and sponsor during the last years of his life. She helped Partch locate studios, including a notorious location in Venice Beach, which was chosen because it was near a liquor store.
Freeman arranged for the production of his final theater work, Delusion of the Fury, which incorporated music from his time in Petaluma, at the University of California, Los Angeles in early 1969.
Harry Partch on the film set for “The Dreamer That Remains” with some of the instruments he built.
Partch photographs – Betty Freeman
Sousa Archives and Center for American Music
University of Illinois at Urbana-Champaign
During his southern California years, Partch had a close brush with something akin to mainstream notoriety. In 1969, Columbia records issued The World of Harry Partch, his first release on a major record label.
Freeman founded the Harry Partch Foundation in 1970 to manage the expenses and administration of Partch’s work. She shared with Partch the purchase of his home in Encinitas, California, and produced the prize-winning documentary The Dreamer that Remains. The soundtrack for The Dreamer that Remains would be his final composition.
Partch retired to Encinitas in 1973. A second edition of “Genesis of a Music” was published in 1974 including additional chapters about work and instruments Partch made since the book’s original publication in 1949.
Harry Partch died of a heart attack 3 September 1974 in Encinitas, California, soon after the completion of principal photography for the documentary The Dreamer that Remains. He was 73.
In 1991, Partch’s journals from June 1935 to February 1936, that he had believed lost or destroyed were discovered and published , musicologist Bob Gilmore published a biography of Partch.
Partch wrote of his musical and artistic his aesthetic:
“The work that I have been doing these many years parallels much in the attitudes and actions of primitive man. He found sound-magic in the common materials around him. He then proceeded to make the vehicle, the instrument, as visually beautiful as he could. Finally, he involved the sound-magic and the visual beauty in his everyday words and experiences, his ritual and drama, in order to lend greater meaning to his life. This is my trinity: sound-magic, visual beauty, experience-ritual.”
https://www.laphil.com/about/watch-and-listen/a-meditation-on-harry-partch-hitchhiking-and-hoboism
https://youtu.be/xPiHjvSCeHw?si=s5sGvamgXwu1A49D
“Let us just pause for a moment and think about how strong an individual came amongst us back then, who worked virtually his entire adult life to bring a personal vision into being,” Danlee Mitchell, assistant to Harry Partch for 20 years and executor of the Harry Partch Estate, wrote on the official Partch website on 24 June 2022
https://www.corporealmeadows.com/about.
https://www.corporealmeadows.com/news-oped/2022/6/24/121-years-ago-in-oakland-california
HARRY PARTCH – The Dreamer That Remains, 1974
Film by Betty Freeman and Stephen Pouliot, conducted by Jack Logan, music direction Danlee Mitchell, sound recordist Mark Hoffman. Filmed on location at San Diego State University, and Encinitas California.
https://youtu.be/nt2cJEQk9kE?si=7qsLg3wZmPfIzpIh
Recordings, Music Videos, Further Reading and Documentaries
The Outsider – The Harry Partch Story
BBC 4 Documentary Harry Partch documentary (2002)
https://youtu.be/xPiHjvSCeHw?si=s5sGvamgXwu1A49D
HARRY PARTCH – Music Studio (Documentary)
A documentary about Partch’s hand-built microtonal instruments. Film by Madeline Tourtelot 1958.
https://youtu.be/rxUrDs_xfoQ?si=mcMLraciPliw_vtG
“Harry Partch’s Instruments”. American Mavericks. American Public Media. February 2003. Archived from the original on June 9, 2004.https://musicmavericks.publicradio.org/features/feature_partch.html.
https://web.archive.org/web/20040609184925/http://musicmavericks.publicradio.org/features/feature_partch.html
Harry Partch Recordings available on Bandcamp and on Amazon from Neuma Records (formerly Neuma Records & Publications), which has been championing exploratory music since 1988.
https://harrypartch.bandcamp.com/album/u-s-highball-1946
https://www.amazon.com/stores/page/7F4BE56C-1DA3-434B-A139-F57C23361F74
Partch, Harry (1974). Genesis of a Music (2 ed.). Da Capo Press. ISBN 0-306-80106-X.
Instruments by Harry Partch
https://en.wikipedia.org/wiki/Instruments_by_Harry_Partch

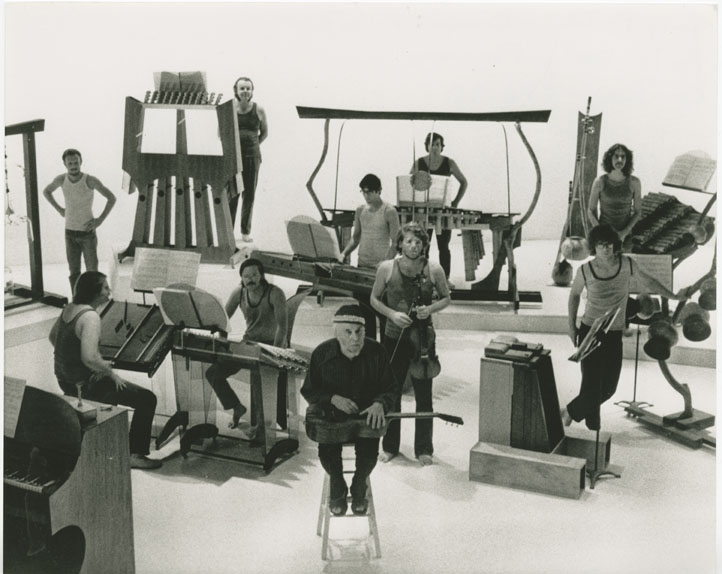
Harry Partch’s original instruments on stage.
A subset of Partch’s original instruments on stage: R to L: Gourd Tree, Cone Gongs, Cloud Chamber Bowls, Adapted Guitar I, Kithara II, Adapted Viola, Bass Marimba, Marimba Eroica, Castor & Pollux, Chromelodeon I & II.
Creative Commons
Sources:
Corporeal Meadows
https://www.corporealmeadows.com
Archive
https://www.corporeal.com/
De Pue, Joanne (2014). “Harry Partch Instrumentarium Takes Up Residency at UW”. University of Washington School of Music.
Gilmore, Bob (1998). Harry Partch: A Biography. Yale University Press. ISBN 0-300-06521-3.
Granade, S. Andrew (2026). The Musical Identities of Harry Partch: History, Theory, Performance. University of Rochester Press. ISBN 978-1648251276.
Harry Partch.com
https://www.harrypartch.com
McGeary, Thomas (2000). “Introduction”. In McGeary, Thomas (ed.). Bitter Music: Collected Journals, Essays, Introductions, and Librettos. University of Illinois Press. pp. xv–xxx. ISBN 978-0-252-06913-0.
https://books.google.com/books?id=_TMKT6ise7kC
Partch, Harry (1901-1974) | University of Illinois Archives
https://archon.library.illinois.edu/archives/?p=creators%2Fcreator&id=2456
Schell, Michael (2017). “Harry Partch: Celebrating a Musical Maverick”. Second
inversion.
https://www.secondinversion.org/2017/05/30/harry-partch-party-celebrating-a-musical-maverick/
Schell, Michael (2018). “Not even Harry Partch can be an island”. Second Inversion.
https://www.secondinversion.org/2018/05/09/not-even-harry-partch-can-be-an-island/
Yang, Mina (2008). “Harry Partch, the Hobo Orientalist”. California Polyphony: Ethnic Voices, Musical Crossroads. University of Illinois Press. pp. 52–57. ISBN 978-0-252-03243-1.